

Abstract
Pulmonary carcinoid tumors, known as pulmonary neuroendocrine tumors, are rare types of lung neoplasms. These tumors, particularly the typical carcinoid type, have a better prognosis compared to other subtypes of lung cancer. However, in some cases, recurrence and metastasis may be observed in patients. In a 24-year-old patient presenting with post-obstructive collapse and hemoptysis in the right upper lobe, a diagnosis of a typical carcinoid tumor was made only two years later. This case highlights the importance of early diagnosis and a multidisciplinary approach in significantly influencing the treatment and prognosis of patients, despite the slow progression of typical carcinoid tumors.
Cover Letter
Summary
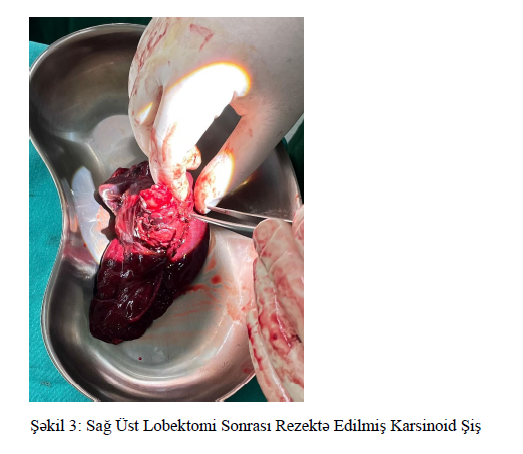
Lung carcinoid tumors are known as pulmonary neuroendocrine tumors and are one of the rare tumors of the lung. These tumors, especially the typical carcinoid type, have a better prognosis compared to other types of lung cancer. However, in some cases, patients may experience recurrence of the disease and metastasis. While the 24-year-old patient had complaints of post-obstructive collapse and hemoptysis in the upper right lung, a typical carcinoid tumor was diagnosed only 2 years later. This fact makes it possible to emphasize that, despite the slow progression of typical carcinoid tumors, early diagnostics and a multidisciplinary approach have a significant impact on the treatment and prognosis of patients. Lung carcinoid tumors are rare tumors that account for 20-30% of all neuroendocrine tumors and about 1-2% of lung-derived cancers. Lung carcinoids have a better survival rate compared to other lung cancer subtypes (1,2). Carcinoid lung tumors are more likely to occur with chest pain, wheezing, hemoptysis, post-obstructive collapse or post-obstructive pneumonia, signs and symptoms. In the clinical case that we are going to present, a low-differentiated (G2) carcinoid tumor of the right lung, diagnosed 1 year after hemoptysis, has been mentioned. Clinical case a 24-year-old patient has been admitted to our clinic with complaints of hemoptysis, chest pain and chest hissing for 2 years. There is no concomitant disease. On physical examination, widespread bilateral wheezing was heard over the lungs. Saturation was measured SpO2 86% in Room Air. In laboratory analyzes, their values were within the normal range. Paag'de taken due to the presence of atelectasis in the upper right chest CT was planned. In chest CT, a 30x32 mm santarli lytic sclerotic lesion in the sternum body was traced,calcifications were traced in the right lung hilus into the right main bronchus obliterating the right upper share bronchus with some indentation, heterogeneously contrasting invasion into the visceral pleura, soft tissue mass measured 34x31 mm at the widest point in sagital images, post-obstructive collapse In the mediastinum, in the neighborhood of the right main bronchus, to the left of the midline at the level of the Carina, lymph nodes (LAP) measured 14x12 mm were monitored in the anterior neighborhood of the left main bronchus. Sclerotic lesion of 3 cm in the Sternum body (metastasis?), in the spleen parenchyma, a nonspecific 6 mm size hypodens structure was traced. (photo 2). The patient was scheduled for a bronchoscopy. During bronchoscopy, a lesion was seen that closed the right upper lobe negative close to the full and extended to the right main Endobronchial Lumen, forceps biopsy was taken. Pathology result carcinoid tumor, reported in the form of NOS. The patient underwent lobectomy, lymphadenectomy with a diagnosis of carcinoid tumor (Figure 3). As a result of the pathology of the resection material, non necrotizing granulomatous inflammation was seen in the typical carcinoid tumor and lymphs. Non necrotizing granulomatous inflammation paraneoplastic syndrome, which may be due to sarcoid-like reaction was thought. Patient 2 months after surgery, chest CT control was planned.
Discussion
Carcinoid tumors of the lung account for < 1% of all lung cancers. Typical carcinoids are usually slow-acting and have a 5-year survival rate of 90%. Metastases of these tumors are very rare. In most cases, pulmonary carcinoid tumors do not show endocrine symptoms at the clinical level. These tumors are usually considered "endocrinologically calm" because they do not produce significant amounts of hormones or bioactive substances that usually cause noticeable clinical effects . Bronchoscopy plays an important role in the diagnosis of lung carcinoids, as these tumors are usually located in a central location and visible during endoscopic evaluation. Biopsy with bronchoscopic assessment is considered the gold standard for the diagnosis of lung carcinoids . In this clinical case, the lesion located in the right upper pay bronchus and occupying the Endobronchial Lumen was diagnosed as a “typical carcinoid tumor”, being confirmed by biopsy. In the pathological examination of the material removed during the operation, non-necrotizing granulomatous inflammation was observed, which caused a sarcoid-like reaction. Although this phenomenon is rare, it is a well-known condition among paraneoplastic syndromes and is related to the response of the immune system in carcinoid tumors.For carcinoids, common neuroendocrine markers, usually including chromogranin and synaptophysin, are positive . The Ki-67 index is very important to distinguish typical from atypical carcinoids,to clarify the degree of differentiation . In our patient, the Ki-67 index(3%) is consistent with the typical carcinoid diagnosis and its slow clinical course. Since lung carcinoids are usually centrally located and localized to the large bronchi, they can also face severe complications such as massive hemoptysis. Our patient had a complaint of minor hemoptysis, which lasted for 2 years. This circumstance once again emphasizes the importance of early diagnosis in the diagnosis and treatment of lung carcinoid tumors. Diagnosis was delayed because the patient's hemoptysis and other nonspecific symptoms, which lasted for two years, were not properly assessed at the initial stage. The slow-progressing nature of carcinoid tumors, nonspecific symptoms and delayed use of diagnostic tools indicate that even a slow-moving tumor can be prevented by paraneoplastic syndrome.
The result
This clinical case shows that although lung carcinoid tumors progress slowly, any delay in diagnosis can negatively affect the quality of life and long-term prognosis of patients. Timely use of bronchoscopic and other advanced diagnostic tools in case of suspected symptoms provides positive results for patients. In addition, early diagnosis with a multidisciplinary approach and appropriate surgical intervention are the basis of effective treatment of lung carcinoid tumors. This approach makes it possible to improve the prognosis of patients and minimize the risks of possible relapse. Early diagnosis, timely intervention and multidisciplinary approach, close follow-up play a key role in the prognosis, morbidity and mortality of carcinoid tumors, including other lung tumors
Figures
Keywords
References
Mənbələr:
1. Bischoff P, Trinks A, Wiederspahn J, Obermayer B, Pett JP, Jurmeister P, Elsner A, Dziodzio T, Rückert JC, Neudecker J, Falk C, Beule D, Sers C, Morkel M, Horst D, Klauschen F, Blüthgen N. The single-cell transcriptional landscape of lung carcinoid tumors. Int J Cancer. 2022 Jun 15;150(12):2058-2071. doi: 10.1002/ijc.33995. Epub 2022 Mar 16. PMID: 35262195.
2. Uprety D, Halfdanarson TR, Molina JR, Leventakos K. Pulmonary Neuroendocrine Tumors: Adjuvant and Systemic Treatments. Curr Treat Options Oncol. 2020 Aug 29;21(11):86. doi: 10.1007/s11864-020-00786-0. PMID: 32862320.
3. Limaiem F, Tariq MA, Ismail U, Wallen JM. Lung Carcinoid Tumors. 2023 Jun 15. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30725765.
4. Filosso PL, Rena O, Donati G, Casadio C, Ruffini E, Papalia E, Oliaro A, Maggi G. Bronchial carcinoid tumors: surgical management and long-term outcome. J Thorac Cardiovasc Surg. 2002 Feb;123(2):303-9. doi: 10.1067/mtc.2002.119886. PMID: 11828290.
5. Langfort R, Rudziński P, Burakowska B. Rozrosty neuroendokrynne płuc. Histologiczne spektrum podtypów, aktualne pglady dotyczace rozpoznawania i leczenia [Pulmonary neuroendocrine tumors. The spectrum of histologic subtypes and current concept on diagnosis and treatment]. Pneumonol Alergol Pol. 2010;78(1):33-46. Polish. PMID: 20162517.
6. Gosain R, Mukherjee S, Yendamuri SS, Iyer R. Management of Typical and Atypical Pulmonary Carcinoids Based on Different Established Guidelines. Cancers (Basel). 2018 Dec 12;10(12):510. doi: 10.3390/cancers10120510. PMID: 30545054; PMCID: PMC6315766
Article Info:
Publication history
Published: 25.Feb.2025
Copyright
© 2022-2025 Azerbaijan İnternal Medicine Society. Published by "Uptodate In Medicine" health sciences publishing. All rights reserved.Related Articles
Viewed: 594