

Abstract
Addison's disease (adrenal insufficiency) is a rare endocrinological disease caused by insufficient secretion of one or more of the glucocorticoid, mineralocorticoid and androgen hormones that should normally be secreted as a result of adrenal insufficiency. This disease occurs at a frequency of 1:100000, with the same equality in women and men, mainly between the ages of 30 and 50
Cover Letter
There is a type of Adrenal insufficiency.
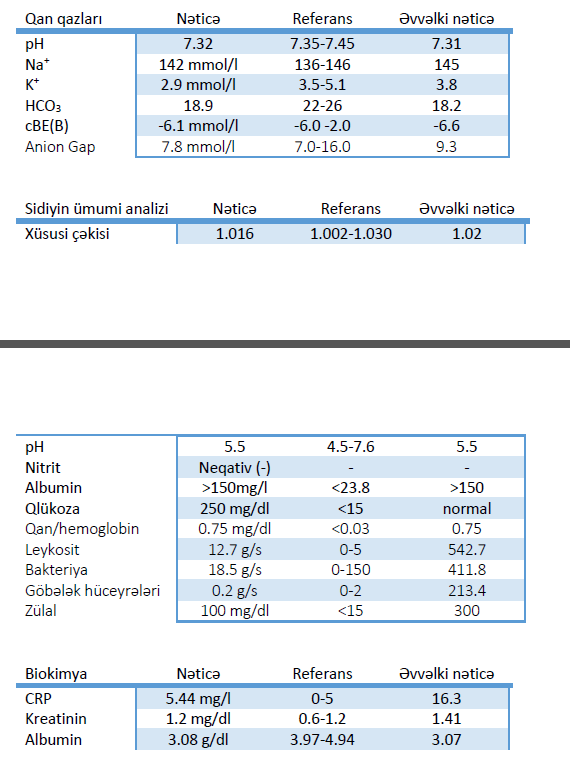
Primary (primary) adrenal insufficiency is Addison's disease as we know it. This disease is when the adrenal cortex is damaged and does not adequately secrete adrenocortical hormones. It appears mainly as a result of autoimmune damage. Secondary (secondary) adrenal insufficiency is caused by insufficient adrenal awareness due to diseases affecting the pituitary and hypothalamus glands, the site of secretion of akth, the adrenal Messenger hormone. In some cases, too, the sudden discontinuation of this drug by people who use corticosteroids to treat diseases such as bronchial asthma and arthritis leads to the appearance of transient secondary adrenal insufficiency. Symptoms of Addison's disease are excessive fatigue, impotence, abdominal pain, muscle and joint pain, dizziness, desire to eat salt, nausea and vomiting, weight loss. These symptoms are seen in patients in the form of lowering blood pressure, darkening of the color on the skin, especially on the head, neck, inside of the hands, on the mucosa (especially on the gums), reduction of hair in the armpits and groin in women, and sexual reluctance. The causes of Addison's disease are most often attributed to the autoimmune process. Other causes include tuberculosis, infectious diseases, bleeding in the adrenal glands, and different types of cancer metastasizing to the adrenal glands. Addison's crisis is a shock that develops in connection with adrenal insufficiency and is life-threatening. Severe malaise, nausea, hypotonia, vomiting, abdominal pain, clouding of consciousness, loss of fluids and electrolytes are followed. Sodium and sugar in the blood decrease. There may also be a potassium elevation. Basically, in situations (physical stress, surgical stress, trauma and infection) that cause stress in the body, Addison's crisis is. The clinical case shown below refers to the incidence of Addison's crisis when investigating the cause of acute renal failure in a patient suppressed by a diagnosis of acute renal failure. Clinical case. A 59-year-old male patient was admitted to the hospital on 07.12.2023 with complaints of chest and abdominal pain, loss of appetite, shortness of breath, general weakness, depressive state, skin color, especially head and neck, darkening of the upper hand, painful urination, decreased urination, nausea and vomiting. He considers himself sick for several months. Earlier, due to the deterioration of his condition, he was admitted to the hospital in the region where he lived, received inpatient and intensive care treatment. For several years he was at the reception of a psychiatrist in connection with the presence of a depressive state. Diabetes mellitus in the Anamnesis, for many years receiving insulinotherapy, there is a narrowing of the urethra. A / T 100/65 mm.c.st, Ps 85 accent/min, SpO 94%. Creatinine was normal when the laboratory received inpatient treatment for the liver 2 months ago, according to the patient as follows. The patient is hospitalized with a diagnosis of hepatorenal syndrome, acute renal failure. Initially, Ringer 500 ml, 8.4% NaHCO3 100 ml, asistan 600 mg, klexan 0.4 tv, NaCl 0.9% 500 ml, ampicide 1.5gx2, Lantus 10 tv treatment are prescribed. Because of the low sugar content in recent days, not bolus insulin, but simply basal insulin (lantus) has been prescribed. After 2 days (09.12.2023), a psychiatrist's consultation is prescribed in connection with the increase in depressive conditions in the patient. Suitable antidepressants are added to the appointment. However, after 2 days (11.12.2023), a deepening of acidosis and hyponatremia in blood gases and an increase in creatinine are seen. The analysis results are as follows: in connection with this, antidepressants are discontinued. One day (12.12.2023) in subsequent analyzes, there was no lag in creatinine and CRP, but no change in acidosis and hyponatremia. To the appointment hypoacid is prescribed 1tabx2 times, allopurinol 100 mg. The low PTH makes us think. Despite the antibiotic therapy carried out, there were no bacteria in the urine, no leukocyte regressions, and a urologist consultation was requested, as urination was observed to be difficult and more painful. The urologist performed a urethratomy operation, tamurin 0.4 mg was added to the appointment. on the left, however, heterogeneous signal changes followed, with a front-back length of 82mm and a transverse length of 51mm. T2 images present mild hyperintense images within the lesion defined on the left side. Hypointense images were recorded in the examination, which was carried out without the introduction of contrast agent in T1-weighted cuts. A pronounced appearance in both adrenal glands can be considered a sign of hypertrophy or a haemorrhagia-hematoma of the adrenal gland in this area. These signs have been noted.
Despite the fact that we have already confirmed adrenal insufficiency in our opinion, we had to wait a day for the results of the analysis.
Results of the analysis on 16.12.2023: immediately hydrocortisone 100 mg+NaCl 0.9% 100 ml bolus was started. Then, every 8 hours, 50 mg of hydrocortisone+NaCl 0.9% 100 ml IV, on the 3rd day, every 12 hours, 50 mg of hydrocortisone+NaCl 0.9% 100 ml IV, on the 4th day, 50 mg of hydrocortisone+NaCl 0.9% 100 ml IV were prescribed. Already on the 5th day, 25 mg of hydrocortisone (genkort) was switched to tablets. Then k+, Na+ , acidosis in the blood was reduced to 17.5 mg hydrocortisone corresponding to the weight followed. Fludrocortisone was not prescribed because the patient did not need additional mineralocorticoids. Blood gases taken during the day already had hyponatremia and acidosis recovery. On 17.12.2023, creatinine decreased to 1.98 mg/dl. The treatment was ongoing. Analyzes on 20.12.2023: improvement was noted in the patient not only in laboratory analyzes, but also in clinical ones. According to the patient, he did not remember what was the last days. He is already feeling better, his depressive state had recovered. His appetite recovered, nausea, vomiting stopped, the horse recovered. Relatively corrections were also noted in skin color. The patient was then continued to be treated as an inpatient by an endocrinologist. We have already confirmed the diagnosis of addison's syndrome. As we know, in the etiology of Addison, autoimmune and tuberculosis disease are most often noted. It also includes infectious and cancer metastases. To know if it was of autoimmune origin, one of the etiological causes, the patient was offered the determination of 21-α - hydroxylase, but they did not take it for financial reasons. In complete abdominal ultrasound conducted on 28.12.2023, both due to etiological investigation and due to registration of diffuse free fluid in the abdominal cavity and fluid in the bilateral pleural space, Quantiferon TB test is requested and the result is negative. The designation also provides lazyx and verashpiron. After 1 Week, complete abdominal ultrasound is repeated. Since the fluid is still at the same level, a consultation with the therapist is prescribed and it is decided that the patient should continue with outpatient control of diuretics even when he is discharged. On 04.01.2024, the patient was discharged, and the laboratory indicators at that time were as follows: when the patient was discharged, he was also advised to make an oncologist appointment in connection with the non-decreasing fluid in the abdominal cavity. The patient was prescribed home magnesium, vitamin D 50,000 8 weeks, genkort 17.5 mg, calcium 1200 mg per day, lantus 10 tv, metforix 1000 mg. 4 days after the patient was discharged, he gave analyzes for CA 19-9 (pancreatic and colon ca) and CEA (carcinoemriogenic antigen). The result: the patient is constantly monitored on an outpatient basis by a nephrologist, therapist and endocrinologist. In August, however, he applies to the therapist for pain in the lower back. In the performed urinary system CT, it is revealed that the mass measured 47x23mm in the left adrenal projection (lymph node? Mts?) is valued internally. A large number of pathologically enlarged lymph nodes are monitored, with the Precaval large measuring 22x19mm and the left paraaortic-preranal large measuring 50x42mm. Both externalparailiac enlarged lymph nodes are noted. In connection with this, the patient is referred to an oncologist. By the decision of the oncologist, the left adrenal gland is surgically removed. After the operation, he receives chemotherapy. In the postoperative check, the laboratory results in October the patient was going on chemotherapy. In postoperative complete abdominal MRI, lesions of the entire parenchyma of the spleen, up to 55x30 mm in size, with irregular contours, heterogeneous structure, cystic character, are initially considered in favor of MTS. In the projection of the left adrenal gland and the tail part of the pancreas, a pathological area with an irregular contour with massive, solid and cystic components is traced. The solid components of the pathological area extend towards the medial and surround the anterior-left paravertebral area at the level of the L5, Th1 vertebrae and the abdominal aorta from the left at the level of the truncus celiacus, below which the extension towards the left psoas muscle. Diffuse thickening up to 12 mm on the walls of the bladder, bumpiness on its inner surface. Solid fluid accumulation with heterogeneous stucture, up to 38 mm thick in the left pleural space. We refer the patient to the oncologist again. But, unfortunately, everything is late for the patient and goes to Mercy.
Figures
Keywords
References
Article Info:
Publication history
Published: 25.Feb.2025
Copyright
© 2022-2025 Azerbaijan İnternal Medicine Society. Published by "Uptodate In Medicine" health sciences publishing. All rights reserved.Related Articles
S.pyogenes eritrogen toksini tərəfindən törədilən skarlatinanın nadir ağırlaşması : pnevmoniya
Viewed: 600